Physician Burnout Is Breaking Medicine — AI Is Offering a Fix
April 22, 2026
How ambient AI assistants are turning the tide on one of healthcare's most intractable crises
The numbers are hard to look away from. 45.2% of all American physicians reported at least one symptom of burnout in a major 2023–2024 national study, according to Stanford Medicine.
While that figure represents meaningful improvement from the 62.8% peak recorded during the COVID-19 pandemic in 2021, it masks a more troubling reality: even at its "best," physician burnout in the United States remains dramatically elevated compared to other professions. After adjusting for age, gender, and work hours, the same Stanford-led study found that physicians are 82.3% more likely to be experiencing burnout than American workers in other occupations.
Physician burnout is no longer a fringe concern for hospital HR departments. It is a systemic crisis with direct consequences for patient safety, care quality, workforce sustainability, and the long-term viability of primary care itself. And for the first time in decades, a credible technological solution, ambient AI, is producing results that were once considered out of reach.
What Is Physician Burnout?
Physician burnout is a state of chronic occupational stress characterized by emotional exhaustion, depersonalization (a sense of detachment from patients and work), and a diminished sense of personal accomplishment. It is clinically distinct from ordinary work stress. Researchers typically measure it using validated instruments such as the Maslach Burnout Inventory, which assesses those three core dimensions.
A 2025 study published in Mayo Clinic Proceedings found that although physician burnout improved modestly between 2021 and 2023, physicians still experience significantly higher burnout and lower satisfaction with work–life balance than other U.S. workers. The study examines trends in physician burnout and work–life integration in the U.S. from 2011 through 2023, comparing physicians with the general working population.
"Many physicians still love what they do, but they just can't keep doing it at this pace in the current practice environment, with its administrative burdens and regulatory burdens, and the proliferation of asynchronous messaging with patients through the electronic health record."
Stanford Shief Wellness Officer Tait Shanafelt
MD
What makes physician burnout particularly insidious is what it does downstream. Evidence consistently shows that it worsens the quality of patient care, increases the risk of medical errors, decreases patient satisfaction, and accelerates physician attrition from the workforce at the exact moment America can least afford to lose doctors. The Association of American Medical Colleges projects a deficit of 86,000 physicians by 2036. Burnout is accelerating that timeline.
As Stanford's chief wellness officer Tait Shanafelt, MD, the lead author of the 2023–2024 national study, put it: "Many physicians still love what they do, but they just can't keep doing it at this pace in the current practice environment, with its administrative burdens and regulatory burdens, and the proliferation of asynchronous messaging with patients through the electronic health record."
Signs of Physician Burnout: What to Watch For
Identifying physician burnout early matters, both for the clinicians experiencing it and for the health systems and practices responsible for their well-being. Common signs include:
- Emotional exhaustion is often the first red flag: a pervasive sense of being depleted at the end of every shift, with little recovery between days.
- This is followed by depersonalization, a creeping emotional distance from patients that can manifest as cynicism, detachment, or a transactional approach to care that feels foreign to a physician's identity and training.
- Other signs include a sense of reduced personal accomplishment — feeling like the work no longer matters or that effort rarely translates to meaningful outcomes.
On a behavioral level, physicians experiencing burnout frequently report spending significant hours on documentation after the workday ends, feeling perpetually rushed during patient visits, and being unable to fully attend to patients during appointments due to competing EHR demands.
The American Medical Association has tracked these trends nationally since 2011, documenting how burnout rates have fluctuated alongside changes in healthcare technology requirements, payment models, and pandemic pressures. Their data confirms what most physicians already know: the causes of burnout are systemic, not individual.
Causes of Physician Burnout: A System Problem, Not a Resilience Problem
One of the most important conceptual shifts in understanding physician burnout is recognizing that it is not a personal failing. As AMA's Christine Sinsky, MD, says: "While burnout manifests in individuals, it originates in systems. Burnout is not the result of a deficiency in resiliency among physicians, rather it is due to the systems in which physicians work."
The causes of physician burnout are well-documented and largely structural:
- EHR documentation burden sits at the top of most physicians' lists. A 2024 study published in the Annals of Family Medicine found that for every 8 hours of patient visits, primary care physicians spent 5.3 additional hours in their EHRs, with 2.1 of those hours devoted specifically to clinical documentation. That math doesn't leave room for a sustainable professional life.
- Fee-for-service payment pressure compounds the problem. To remain financially viable, primary care physicians often must see 20 to 30 patients per day in under-20-minute appointment slots. This structural constraint means that documentation, which can consume half of every visit time, competes directly with the patient interaction itself. Physicians describe feeling like they are on a hamster wheel: always running, always behind, never catching up.
- After-hours work, what physicians bitterly refer to as "pajama time," is the logical consequence. When documentation can't get done during the day, it bleeds into evenings and weekends. This erosion of personal time is one of the most corrosive contributors to long-term burnout and dissatisfaction.
Specialty-specific pressures also shape physician burnout by specialty. The Stanford-led study found that physicians in emergency medicine and general internal medicine face heightened burnout risk, which is concerning given that these are often patients' first point of contact with the healthcare system. Primary care physicians, family physicians, and hospitalists consistently rank among the most burned-out cohorts nationally.
Physician Burnout Statistics: The Scale of the Crisis
For anyone seeking to understand the scale of what American medicine is facing, the physician burnout statistics are sobering:
- 45.2% of physicians reported at least one burnout symptom in the most recent national study (2023–2024), per Stanford Medicine — down from 62.8% in 2021 but still far above pre-pandemic levels
- Physicians are 82.3% more likely to experience burnout than other American workers, after adjusting for comparable factors
- Female physicians face roughly 27% higher burnout risk than male physicians, even after controlling for age, specialty, and hours
- For every 8 hours of patient visits, primary care physicians spend 5.3 hours in the EHR, with 2.1 hours on clinical documentation alone
- The U.S. faces a projected shortage of 86,000 physicians by 2036, with burnout-driven attrition a leading accelerant
Physician assistant burnout follows parallel patterns, with PAs in high-acuity or high-volume settings reporting comparable levels of emotional exhaustion and role strain to their physician colleagues. The burnout crisis is not confined to MDs.
Physician Burnout by Specialty: Who Is Most Affected?
While burnout touches physicians across virtually every specialty, the burden is not evenly distributed. Emergency medicine physicians consistently rank among the highest for burnout risk, driven by unpredictable patient loads, life-or-death time pressure, and high emotional intensity. General internal medicine, family medicine, and hospitalist medicine also show elevated rates, shaped heavily by documentation demands and the weight of managing complex chronic disease panels under fee-for-service constraints.
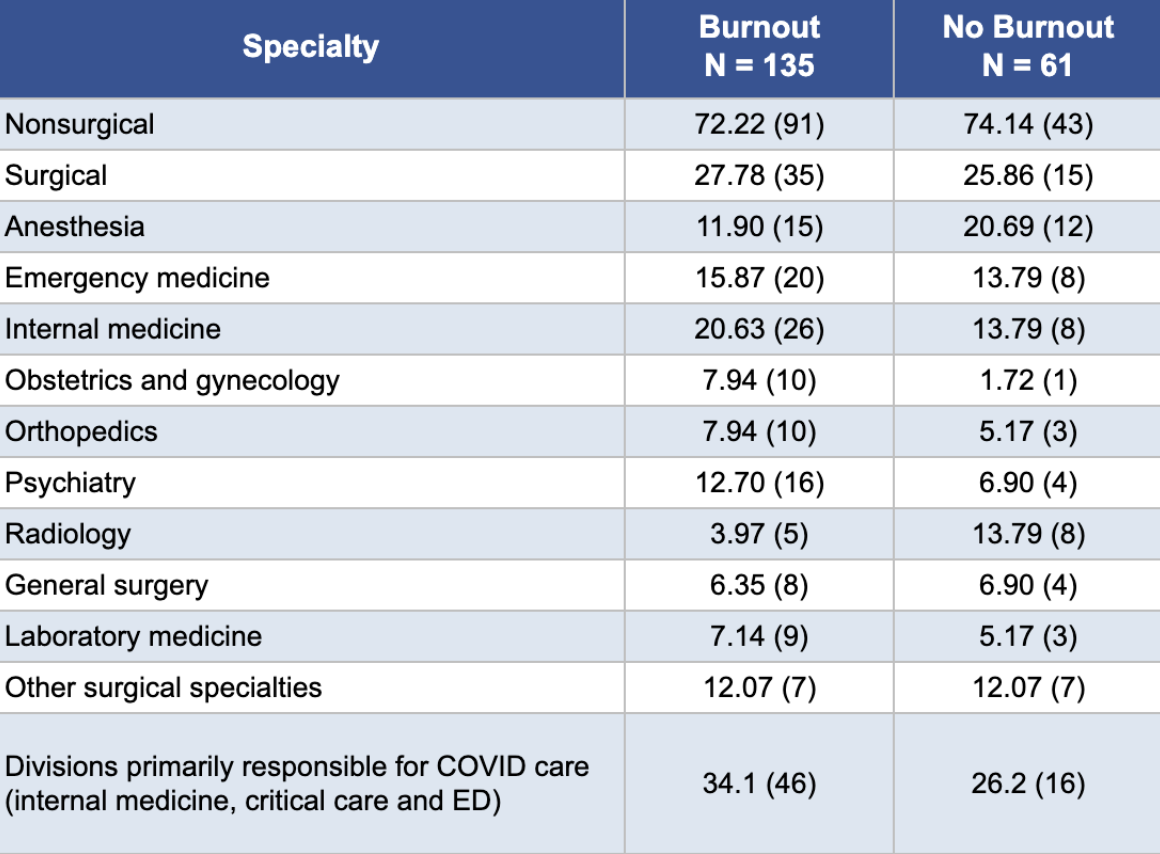
Data source: Differences in Physician Burnout by Specialty: A Cross-Sectional Survey
Specialties with greater procedural autonomy and clearer episodic care cycles, such as certain surgical subspecialties, tend to report somewhat lower burnout, though no specialty is immune. Physician burnout by specialty data consistently points back to the same root causes: administrative overhead, EHR burden, and insufficient time for meaningful patient engagement.
Physician Burnout Treatment and Solutions: What Actually Works
The field of physician burnout treatment has matured considerably over the past decade. Individual-level interventions, mindfulness programs, resilience training, and wellness apps have their place, but the research is clear: durable relief requires system-level change. Reducing the structural sources of burden is what moves the needle.
"Although advocates for physician wellness often promote the idea of doctors improving their individual resiliency to the pressures of their profession, there is increasing recognition that addressing burnout in medicine will require changes at the systems level."
Roger Collier
The most promising developments in reducing physician burnout center on three levers: reforming documentation workflows, improving EHR usability, and deploying AI to absorb administrative labor. Of these, AI-powered ambient documentation has emerged as the most rapidly scalable and measurably impactful.
- Reforming documentation workflows addresses the sheer volume of charting, prior authorizations, and after-hours paperwork that now consume a significant portion of a physician's day, time that was once spent in direct patient care. Structural changes here include streamlining note requirements, reducing redundant data entry, and redesigning team-based workflows so that clinical documentation is shared more equitably across the care team rather than funneled exclusively to the physician.
- Improving EHR usability targets a different frustration: the clunky, fragmented interfaces that turn routine charting into an obstacle course. Many electronic health record systems were designed around billing compliance rather than clinical efficiency, resulting in interfaces that require excessive clicks, bury critical information, and interrupt the natural flow of patient encounters. Investments in better UX design, customizable templates, and tighter integration between systems can meaningfully reduce the cognitive friction clinicians experience with every login.
- Deploying AI to absorb administrative labor goes further still, using machine learning and natural language processing to automate tasks that previously demanded human attention, drafting referral letters, processing inbox messages, surfacing relevant patient history, and flagging coding errors. Rather than simply reorganizing existing work, AI has the potential to eliminate entire categories of low-value tasks that have accumulated over decades of regulatory and billing complexity.
Of these three levers, AI-powered ambient documentation is by far the most promising, due to its pace of adoption and its direct impact on the patient encounter. The technology works by passively listening to a clinical conversation, through a smartphone or dedicated device, and then generating a structured clinical note in real time. Using large language models trained on medical language, the system transcribes the visit, identifies relevant clinical elements, and organizes them into the appropriate sections of a SOAP note or equivalent format, ready for physician review and sign-off.
The result is that clinicians can be fully present with their patients rather than glancing at a screen, and the hours of after-hours charting that drive so much burnout can collapse into minutes of light editing. For example, Suki customers have reported reductions in documentation time of 40% or more, along with 81% improvements in physician satisfaction, and 60% reduction in feelings of burnout.
How Ambient AI Is Transforming Physician Burnout: The Research
In February 2025, Phyx Primary Care, an independent, non-profit innovation lab that evaluates emerging healthcare technologies, published a landmark study examining what happens when primary care physicians adopt an ambient AI assistant for clinical documentation. Their partner for the evaluation was Suki, an AI platform purpose-built for clinical environments.
The results were, by any objective measure, extraordinary.
Across a cohort of 116 primary care providers at 37 practice locations spanning independent practices, primary care organizations, and large health systems, the Phyx team tracked changes in what they call the Primary Care Vital Signs®: burnout, satisfaction, visit time, care time, after-hours work, and documentation burden.
After more than 30 days of using Suki, physicians reported:
- 60% reduction in burnout (statistically significant, p<0.001)
- 81% increase in physician satisfaction (p<0.001)
- 41% reduction in documentation time per note — from 13.8 minutes to 8.2 minutes
- 37% decrease in after-hours work — saving physicians approximately 48 minutes per day
- 32% fewer "rushed" visits
- 46% more notes completed before the next patient
The burnout numbers deserve special attention. Before adopting the AI assistant, the cohort's mean burnout score sat at 2.7 on a five-point scale, hovering at the edge of "I am definitely burning out." After using the tool, it dropped to 2.0, representing "I am under stress, but I don't feel burned out." Among the subset of physicians who entered the study already experiencing burnout, the mean score fell from 3.4 to 2.4. The distribution shifted visibly and meaningfully.
Phyx's authors were candid about one surprising aspect of the data: the magnitude of improvement in burnout and satisfaction appeared disproportionate to the raw time savings alone. Their hypothesis: "Respondents may have felt overdue for any burden relief and that the magical nature and impact of the ambient AI assistant gave them immediate relief and much-needed hope."
Physicians in the study described the experience in language that was hard to reduce to bullet points:
"It has fundamentally changed my approach to seeing patients. I don't worry about getting details documented during the visit because I know the AI is doing it for me. I can sit and face the patient most of the time. They like that better."
"Documentation has been much less burdensome. Much less of an albatross around the neck of myself and my providers. Has decreased cognitive burden and warded off burnout."
"It has helped me to have more time with my children at home."
The Net Promoter Score among burned-out physicians in the cohort was 62 — 70% promoters, 8% detractors. For a technology deployed in a population of clinicians conditioned by years of disappointing health IT, that number is remarkable.
Real-World Results: How Health Systems Are Reducing Physician Burnout with Suki
The Phyx data reflects broader patterns playing out at health systems across the country.
Franciscan Missionaries of Our Lady Health System (FMOLHS), a leading regional health system serving Louisiana and Mississippi, partnered with Suki in late 2023 after internal analytics confirmed that providers were drowning in EHR documentation. The results from their pilot were striking: 100% of surveyed users reported improved work-life balance, 48% reported reduced cognitive burden, and EHR data showed a 65% drop in after-hours note completion. Revenue capture also improved as encounters were coded at higher E/M levels, thanks to the completeness and detail of AI-generated notes. Some clinicians voluntarily increased their patient volumes after regaining time in their schedules.
"Suki has consistently been a true partner," said Jenny Smith, Senior Director of Digital Health at FMOLHS. "They get the problems we're trying to solve and bring true solutions to those problems."
Rush University Medical Center, one of the country's most prominent academic health systems, has also partnered with Suki (https://www.healthcareitnews.com/news/rush-partners-suki-tackle-physician-burnout) to address physician burnout, recognizing that ambient AI represents a structural solution to a structural problem, not another wellness perk layered on top of an unchanged system.
"After using other AI documentation solutions, Suki stood out to us for its depth of integration with Epic, ability to do more than documentation, and competitive cost," said Dr. Bina Desai, Rush's chief medical informatics officer. "We understand the profound impact that AI solutions can have on our clinicians as well as patient care."
What Makes an Ambient AI Assistant Different from a Scribe App
Not all documentation tools are created equal, and healthcare leaders evaluating physician burnout solutions should understand the distinction. Simple ambient scribes, often described as "LLM wrappers", transcribe physician-patient conversations into text with minimal EHR integration. They can help with note generation, but their utility stops there.
True AI clinical assistants, like Suki, operate at a fundamentally different level. They employ multiple layers of AI — automated speech recognition, natural language processing for semantic mapping, and large language models for note generation — all tightly integrated with the EHR. This means the AI understands not just what was said, but what it means clinically: distinguishing a patient complaint from a physician command, recognizing that "hypertension" and "high blood pressure" refer to the same condition, and routing content into the correct sections of a structured clinical note.
Crucially, these platforms are built specifically to extend far beyond documentation. From chart review to coding assistance, inbox management, order entry support, and medication reconciliation, a true AI clinical assistant like Suki is designed to help with all the administrative tasks that tend to consume much of a physician's day. The promise of AI in healthcare is to function as a comprehensive solution that puts an end to endless admin. That’s why Suki built its AI infrastructure to power every healthcare workflow, making more focused patient care possible.
Trust and physician control are central to how these systems are designed. Notes are never auto-submitted; physicians review, edit, and approve every note before it enters the chart. Every AI-generated element is fully editable. The physician retains complete authority.
The Path Forward: Physician Burnout Solutions That Scale
Physician burnout is not going to be solved by yoga classes or mindfulness workshops. The evidence — from the AMA's decades of national research, from the Stanford-led longitudinal studies, from the Phyx Innovation Lab, and from health systems deploying ambient AI at scale — points consistently toward the same conclusion: the path forward runs through structural change in how physicians spend their time.
Ambient AI assistants represent the first technology in a generation that demonstrably shifts the burden of clinical administration away from physicians and back to where it belongs, as a byproduct of good patient care rather than an obstacle to it. When documentation becomes a direct output of the physician-patient conversation rather than a separate after-hours task, something fundamental changes. The richer the clinical encounter, the better the note. The better the note, the better the coding, the better the reimbursement, and — critically — the better the care.
For physician burnout treatment that actually works at scale, the prescription is becoming clearer: give physicians back their time, their attention, and their patients. The technology to do it is here.
To learn more about Suki’s Ambient Clinical Intelligence and its impact on physician burnout, explore the Phyx Primary Care Report, the FMOLHS case study, or reach out and get in touch with our team.