Clinical Documentation in the Age of Ambient AI
July 14, 2026
Why the Clinical Note is the Pulse of Healthcare
The clinical note is far more than a post-visit administrative task; it is the fundamental vehicle for the delivery and continuity of healthcare. Its importance is rooted in three critical functions:
- A Communication Bridge: It translates complex clinical encounters into actionable plans for patients, caregivers, and multidisciplinary care teams, ensuring everyone is aligned on the path to recovery.
- The Basis for Reimbursement: It serves as the primary evidence for billing, documenting the complexity and specific interventions of the care provided.
- A Legal Anchor: It acts as the definitive legal record of care, protecting both the patient and the clinician by detailing the decision-making process and clinical rationale.

The Cost of a "Poor" Note: Clinical, Financial, and Legal Realities
When documentation falls short, the repercussions ripple across the entire health system. The following data points highlight the specific vulnerabilities created by sub-optimal notes.
1. The Clinical Safety Gap: Inaccuracy and Omission
Without the support of dedicated documentation tools, clinical notes are frequently plagued by inaccuracies and missing data. Research comparing physician notes to audio recordings of encounters found that roughly 90% of notes contained at least one error, including "errors of commission"—where findings were charted that never actually occurred—and significant "errors of omission" regarding the patient’s medical history. [1,2]
2. The Financial Drain: Unbilled Care and Shrinking Margins
Hardworking clinicians often juggle intense administrative burdens alongside back-to-back patient visits, leading to notes that lack the granular detail required for accurate coding. This results in a significant loss of specificity, where high-complexity care is billed at lower levels or missed entirely. This financial hit is particularly devastating for community and non-academic health systems, which deliver approximately 80% of healthcare in the U.S. and are currently facing a "perfect storm" of rising labor costs, high inflation, and stagnant Medicare reimbursement rates. [3,4] For these institutions—many of which operate on razor-thin margins—poor documentation is not just an administrative lapse; it is a threat to their ability to recruit and retain staff in an increasingly competitive market.
3. The Legal and Ethical Risk: Accountability and Trust
From a legal perspective, a poor-quality or missing note leaves a clinician defenseless and a patient without a voice. Documentation serves as the only objective evidence in cases of medical necessity or liability; without it, there is no way for patients to hold clinicians accountable, nor for clinicians to prove they met the standard of care. Beyond the courtroom, high-quality documentation is essential for building trust and transparency. When a patient reads a note that accurately reflects their experience, it reinforces the therapeutic alliance; when a note is incoherent or missing, that trust evaporates. [5]
When documentation falls short, the repercussions ripple across the entire health system.
Sudha Jayaraman
The Challenge: The Lack of a "Gold Standard"
One of the greatest hurdles in clinical documentation is that there is no universal "gold standard." Every note is as unique as the clinician who writes it, reflecting their specific knowledge, individual thought process, and the unique nuances of the patient-clinician interaction. Because notes vary so widely across specialties, standardizing quality without stifling clinical judgment has remained an elusive goal.
How Ambient AI Redefines the Standard
Ambient AI solves the documentation crisis by capturing the encounter as it happens, ensuring the note meets the high standards of modern medicine through three key pillars:
- Unmatched Specificity: By integrating real-time dialogue with EHR data, AI can distinguish between general and specific diagnoses—for example, documenting "Type 2 Diabetes with Peripheral Neuropathy" instead of a generic "DM2."
- Objective Accuracy: Because the capture is real-time, the system does not rely on a clinician’s memory at the end of a long day of seeing 20+ patients. It records the details exactly as they were discussed.
- Seamless Speed: The automation of the note-taking process allows for immediate completion, removing the "pajama time" burden and ensuring the record is available for the next care transition without delay.

Measuring Success: What is the Benchmark?
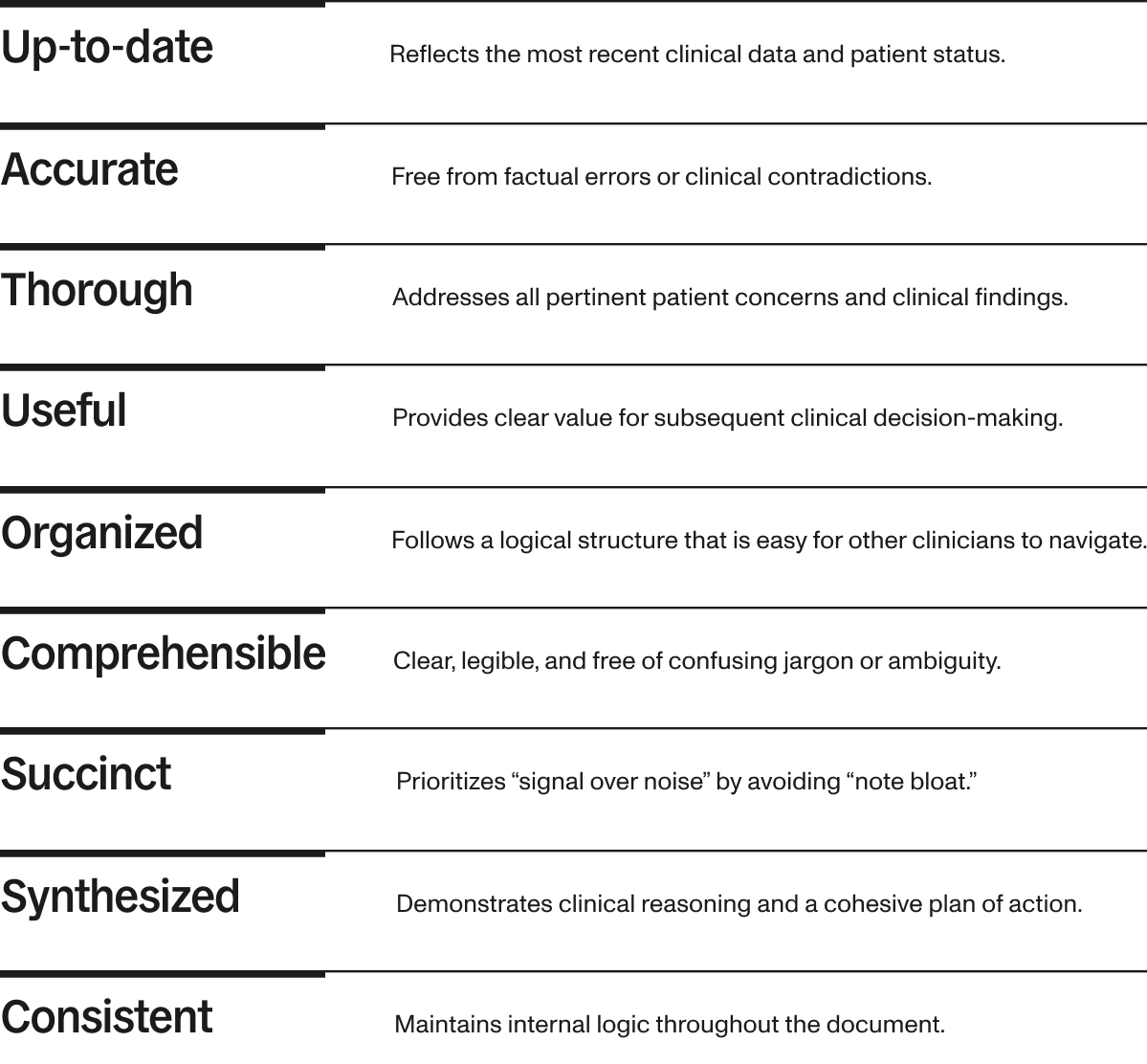
While there is no "gold standard" for assessing quality of an ambient AI-generated note, the Physician Documentation Quality Instrument (PDQI-9) is widely used for assessing clinical note quality.[6] Developed to move beyond simple checklists, it uses nine domains to measure the quality of documentation. [7]
Is PDQI-9 the Ultimate Framework for Note Quality?
Although the PDQI-9 has been used in numerous papers on note quality, its utility is suspect.[8] From a scientific standpoint, it has several flaws. Because it relies heavily on the subjective interpretation of the reviewer, inter-rater reliability can vary significantly. The domains are vague and not actionable. It has not been validated across all specialties or healthcare settings. While the PDQI-9 provides a necessary baseline for contemporary quality checks, the evolution of documentation technology suggests that a more objective, data-driven framework may be required to truly define what makes a clinical note "excellent."
Sudha Jayaraman, Medical Director, Clinical Strategy and Research
References
- Weiner SJ, Wang S, Kelly B, Sharma G, Schwartz A. How accurate is the medical record? A comparison of the physician's note with a concealed audio recording in unannounced standardized patient encounters. J Am Med Inform Assoc. 2020 May 1;27(5):770-775. doi: 10.1093/jamia/ocaa027. PMID: 32330258; PMCID: PMC7647276. https://pmc.ncbi.nlm.nih.gov/articles/PMC7647276/
- Edwards ST, Neri PM, Volk LA, Schiff GD, Bates DW. Association of note quality and quality of care: a cross-sectional study. BMJ Qual Saf. 2014 May;23(5):406-13. doi: 10.1136/bmjqs-2013-002194. Epub 2013 Nov 28. PMID: 24287259. https://pubmed.ncbi.nlm.nih.gov/24287259/
- https://www.ahrq.gov/chsp/data-resources/compendium.html
- https://www.aha.org/press-releases/2025-04-30-new-aha-report-hospitals-and-health-systems-squeezed-persistent-economic-challenges#:~:text=%E2%80%9CThis%20report%20should%20serve%20as,President%20and%20CEO%20Rick%20Pollack
- Ghaith S, Moore GP, Colbenson KM, Lindor RA. Charting Practices to Protect Against Malpractice: Case Reviews and Learning Points. West J Emerg Med. 2022 Apr 28;23(3):412-417. doi: 10.5811/westjem.2022.1.53894. PMID: 35679491; PMCID: PMC9183775. https://pmc.ncbi.nlm.nih.gov/articles/PMC9183775/
- Weiner M, Flanagan ME, Ernst K, Cottingham AH, Rattray NA, Franks Z, Savoy AW, Lee JL, Frankel RM. Accuracy, thoroughness, and quality of outpatient primary care documentation in the U.S. Department of Veterans Affairs. BMC Prim Care. 2024 Jul 18;25(1):262. doi: 10.1186/s12875-024-02501-6. PMID: 39026167; PMCID: PMC11264844. https://pubmed.ncbi.nlm.nih.gov/39026167/
- Stetson PD, Morrison FP, Bakken S, Johnson SB; eNote Research Team. Preliminary development of the physician documentation quality instrument. J Am Med Inform Assoc. 2008 Jul-Aug;15(4):534-41. doi: 10.1197/jamia.M2404. Epub 2008 Apr 24. PMID: 18436914; PMCID: PMC2442259. https://pmc.ncbi.nlm.nih.gov/articles/PMC2442259/
- Walker KJ, Wang A, Dunlop W, Rodda H, Ben-Meir M, Staples M. The 9-Item Physician Documentation Quality Instrument (PDQI-9) score is not useful in evaluating EMR (scribe) note quality in Emergency Medicine. Appl Clin Inform. 2017 Sep 26;8(3):981-993. doi: 10.4338/ACI2017050080. PMID: 28956888; PMCID: PMC6220701. https://pubmed.ncbi.nlm.nih.gov/28956888/